KIDS - BROKEN ANKLE (TIBIA FRACTURE)
WITH GROWTH PLATE INJURY
our website is for educational purposes only. the information provided is not a substitution for seeing a medical doctor. for the treatment of a medical condition, see your doctor. we update the site frequently but medicine also changes frequently.
What is a Broken Ankle with Growth Plate Injury?
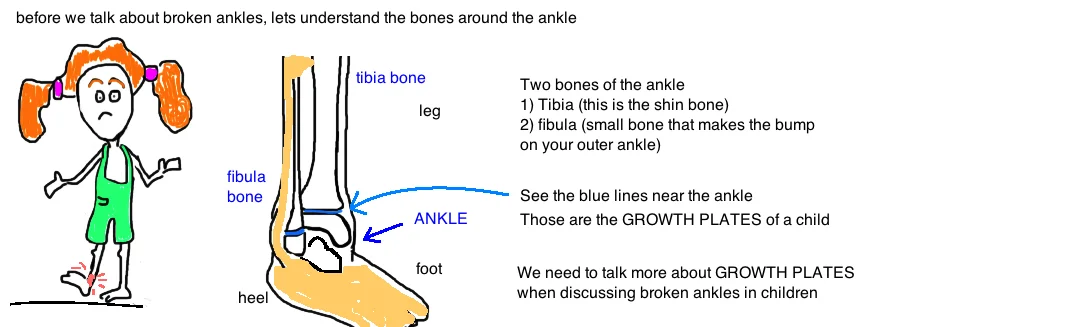
A broken ankle (distal tibia fracture) is common in both kids and adults. But kids and adults break their ankle in different ways.
Most of the time we break our bones at the weak spots. The chinks in the armor. In kids, the break occurs near or through the growth plate (also called the "physis").
A growth plate is a weak area in the bone of kids because its made of baby bone (aka "immature bone").
The bones in your legs and arms start out as cartilage, and then get covered by calcium and becomes normal bone. We get taller by this process. This process occurs at the growth plate (called "enchondral ossification"...look at picture 2 to see the process occurring at a growth plate). The problem is that cartilage isn't as strong as bone, and therefore its common to break a bone right at the growth plate.

Breaking a growth plate is a concern for every kid and parent because we don’t want our growth plates to stop working. We want to keep growing! The good news is that its uncommon to permanently damage our growth plates after a fracture (unless its a very bad injury), usually the growth plate heals like the rest of you and then goes on doing its job.
Occasionally the growth plate stops working after an injury and kids are at risk for having one leg longer than the other. Doctors can identify the kids at risk for this (although they can never predict it 100%). The pattern of growth plate injury can help determine the risk of permanent injury (see picture below). There are a few basic patterns (based on the Salter-Harris Classification). The higher the classification number, the greater the risk of permanent growth plate injury.

Children can experience any of the above types of growth plate injuries. But the most common is a Type 2...meaning the break goes through the growth plate but not into the ankle joint, rather the crack exits into the tibia bone forming whats called a Thurston-Holland spike fragment. This injury is common in sports (especially football, when someone falls onto the foot) or in a motor vehicle collision.
Teenagers however get very unique types of broken ankles.
When we become adults, the growth plates "fuse", which means they stop working and we stop growing.
Because teenagers are almost full adults, their growth plates are partially fused. The ankle growth plate (distal tibia) fuses centrally first, then progresses medially, and finally laterally. This pattern of fusion gives rise to two unique fracture patterns which occur only in teenagers when the distal tibial growth plate is fusing (growth is slowly stopping) but not completely fused (like in adults).
The first is called Tillux Fracture. In ateenager, the outside of the ankle (the lateral tibial physis) is the last area to fuse and it remains a weak spot....a bad ankle injury causes the anterior tibiofibular ligament to pulls off a chunk of tibia (this is known as an avulsion injury). Its considered a Type 3 Salter Harris Fracture because the break goes from the growth plate into the ankle joint. These often need surgery to repair.
The second fracture pattern to discuss is the Triplane Fracture, which occurs in three planes, essentially the fracture starts outside the growth plate, goes through the growth plate, travels across the growth plate, and then enters the ankle joint. These are usually pretty high energy fractures and often need surgery for correction.
How is a Broken Ankle with Growth Plate Injury diagnosed?
Doctors are suspicious for a broken ankle when a kid comes in reporting twisting or falling onto their ankle and are now unable to bear weight on the leg. The ankle is usually tender and swollen.
A doctor will order basic x-rays, which are the best way to diagnose a broken ankle. Its uncommon to need a CAT scan (unless the bone is really banged up). MRIs arent required because x-rays give doctors a great view of the injured bone, and they can plan their treatment with x-rays alone.

How is a Broken Ankle with Growth Plate Injury treated?
Doctors want a straight leg and an ankle with normal alignment. When the ankle breaks, the leg needs to be straightened back out, and this is done in different ways depending on the severity of the injury.
In the emergency room or operating room, the child is often put to sleep because its painful to straighten out a broken bone... the bone is pulled straight and then put into a cast to hold it straight.
Many times a cast alone can hold the break in position while it heals. The leg will then be secured in a long-leg cast for 8-10 weeks, and the is not allowed to put any weight on the leg while it heals.
Sometimes the break needs to be fixed in the Operating room with a small screw. When the crack in the bone travels into the ankle joint, their is a higher risk for needing surgery because the joint surface needs to be perfectly re-aligned in order to minimize risk of future arthritis.

What is the long term outcome?
The biggest factor that determines risk of growth plate damage is how the injury occurred:
Was it a high-energy injury (like a car crash)? or a low-energy mechanism (like a sports injury)?
In general, high energy injuries have a higher risk of premature closure, sometimes up to 85%, while low energy (like sports injuries) have a 10% risk or lower. Other factors to determine risk of growth plate injury include: the amount of growth plate displacement (did it move out of position?) before and after the injury is treated.
One study showed that >3 mm of remaining displacement significantly increased the risk for growth plate injury (stops working). The concern is that sometimes soft tissue (like periosteum gets caught between the fracture preventing it from being re-aligned). Animal studies have shown that presence of periostem between bone does not cause an increased incidence of bar formation (aka premature closure of the growth plate). However, its always a concern. Sometimes it’s a problem if the growth plate closes early, but sometimes it doesn’t even matter. Most people walk around with slightly asymmetric legs, and we don’t even notice (in the same way that our feet are not exactly the same size) but it only becomes a problem once the legs are different enough that we walk with a limp. Usually any difference less 2 cm can be treated with a shoe insert. Once the difference goes beyond that, surgery is often used to correct the limb lengths. The femur and tibia growth at predictable speeds around the knee (9mm/year and 6 mm/year, respectively) and we can temporarily stop growth in the opposite leg of the injury, so that they will reach the same length. But in general, surgery is not necessary as long as the fracture doesn’t enter the joint, and doesn’t remain angulated to strongly after its restraightened.