ACHILLES TENDON RUPTURE
(torn achilles tendon)
our website is for educational purposes only. the information provided is not a substitution for seeing a medical doctor. for the treatment of a medical condition, see your doctor. we update the site frequently but medicine also changes frequently. thus the information on this site may not be current or accurate.
related talks: achilles tendonitis; high ankle sprain; low ankle sprain
What is an Achilles Tendon Rupture?
The Achilles tendon is the thickest tendon in the body. It experiences forces 6-10 times a persons body weight during running. The Achilles tendon is formed from you calf muscles and it attaches to your heel bone, as the calf muscle contracts it helps your foot to push off the ground.
Rupture of this tendon mostly occurs in the "Weekend Warrior" population (referring to men and women between 30-50 years old that work desk jobs all week and then vigorously exercise on weekends to make up for lost time). The tendon ruptures during rapid ankle flexion (hyper-dorsiflexion), such as landing awkwardly while playing basketball.

The rupture usually occurs 2-6 cm from its insertion onto the heel bone, this area is a weak link in the tendon because this area doesnt get a lot nutrients due to poor blood flow here. The delivery of nutrients is essential to allow the tendon to heal all the tiny micro-tears that it experiences from daily use (which you dont even feel). Even though over 95% of people have no symptoms of Achilles tendon pain before the injury, over 95% of tendons show signs of degenerative changes on MRI (meaning the tendon wasnt in great shape before tearing, its like one of those older rubber-bands that snaps a little too easily).
How is Achilles Tendon Rupture diagnosed?
An Achilles tendon rupture can be diagnosed right after its torn ("Acute Rupture") or its sometimes not noticed until weeks or months after rupture (called a "chronic rupture").
A person coming in with an acute rupture will describe a recent injury that occured during exercise, where they heard a "pop" and then experienced significant heel and ankle pain, as well as weakness with push off.
On examination there is often a gap that can be felt where the tendon used to be (just above the heel bone). Also, squeezing the calf muscle should flex the foot downward (thats what the muscle wants to do), but if the foot fails to move, its likely that the muscle isnt attached to the heel bone because of the tendon rupture. This test is called the "Thompson Test" and is helpful for diagnosing the injury.
Unfortunately about 25% of cases are initially mistaken for a simple ankle sprain. The Achilles tear will be inappropriately treated, leading to a delay in diagnosis, and as we will describe below, the treatment changes between an acute vs. a chronic tendon rupture.
How is Achilles Tendon Rupture treated?
A ruptured Achilles tendon is treated based on a person's age, their expectations and activity level, as well as how long ago the injury occurred (acute vs. chronic). The earlier the treatment gets started, the better chance the tendon will heal strongly and will not re-rupture.
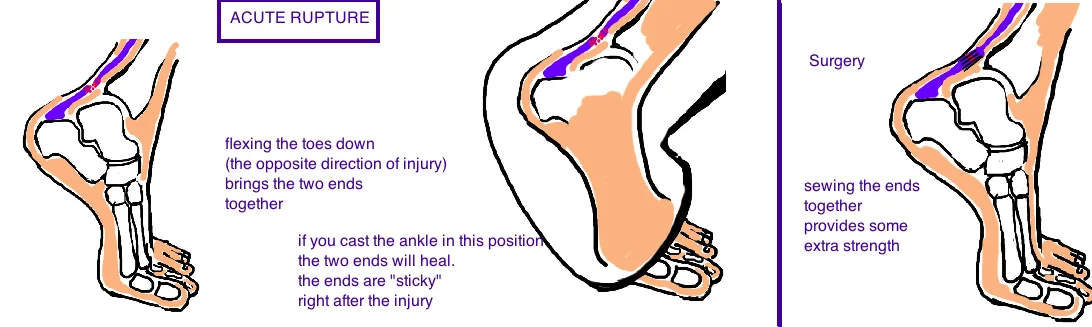
An Acute Rupture means the injury occurred within the last 6 weeks. This injury can be treated with surgical repair or with nonsurgical treatment.
Nonsurgical treatment has undergone a significant change in recent years. The classic treatment was a fiberglass cast (starting just below the knee and going down to the toes) that positioned the foot & ankle pointing to the ground (called plantar-flexion). This position pushes the torn ends of the tendon close together so they heal. This treatment has been effective for many people, but the re-rupture rate is about 10% (about double that of surgery). Now its a common misnomer to think that a ruptured tendon will roll all the way up the leg like window blinds. In truth, the achilles tendon is covered by a sheath (called the paratenon) which doesn't tear during the injury and actually prevents the tendon from retracting more than 1.5 cm (not too far, so when the foot is repositioned this gap becomes minimal).
Recently studies show that instead of protecting the injured ankle in a cast for 6 weeks, a treatment of early rehabilitation in a brace, and early weight bearing provides better healing and reduces re-rupture rates to levels similar to surgical treatment. Now this sounds counterintuitive: you would think the tendon needs to be protected while it heals, but this isnt completely true. The idea is that tendons respond well to stimulation when healing. They want to be motivated by a mild and controlled stress which encourages it to become stronger (almost like working out). The great long-term results has pushed many orthopedic surgeons to recommend nonsurgical treatment instead of surgical repair which they would have recommended 10 years ago.
Surgery on an acute rupture will tie the two ends back together. Here the rate of rerupture is only 3.5% (better than nonoperative treatment) and some studies show better recovery of muscle strength. However, certain complications can only occur with surgery (like 4% of cases become infected, which can lead to severe consequences).
Its best to recognize that both treatments have pros and cons, and people must select a treatment that best fits them. The advantages of surgery probably benefit competitive athletes the most, because they put the highest stress on their tendon and therefore have a higher risk of re-rupture to begin with. However, in the average active person, recent studies all suggest functional bracing with early rehabilitation has a risk of re-rupture equal to surgery but doesnt have any of the pain and complications associated with surgery.
Also both treatments require an extensive rehabilitation process and both treatments allow patients return to running activities between 4-6 months (it takes a while to recover no matter what you decide).
An old injury is called a "chronic rupture" and its given this distinction if the injury occurred more than 6 weeks ago. By the time its discovered, the tendon has already finished most of its healing, and unfortunately, it probably didn't heal in the right position, and the two ends almost certainly didn't reconnect. The window for nonsurgical treatment has passed because the two ends are comfortable in their new position and they don't stick back together like an acute rupture. Therefore, surgery is almost always needed to correct the injury. There are 2 ways to address this problem. If the gap between the ends is small (less than 4 cm), then new edges can be created by trimming back the nonsticky ends to create newer and sticker tendon ends that can be sown together. If the gap is larger (over 4 cm) then these two ends cannot be trimmed because they will never reach each other to be reconnected. In this case, the Achilles tendon needs to be reconstructed by borrowing from another tendon of the leg (usually one of the tendons that flexes the big toe).

Chronic Achilles Tendon Rupture, Old Achilles Tear: Treated with surgery: FHL Transfer
What is the long term outcome?
Re-rupture is a real concern with this injury. The tendon tears initially because its not completely healthy, and you can imagine that things arent getting any better after its torn. Re-rupture typically occurs within the first 12 weeks of healing when then tendon is in the middle of healing and a time in rehab when the tendon is starting to experience stress but it has not completely healed.
It would be reasonable to wonder: "Why not just wait until the 12 weeks have passed before starting to work the tendon again?". The problem with keeping a cast on for too long, is that the tendon becomes too stiff, and the ankle will loose the ability to flex up and down, and this may cause a permanent problem with walking.
For a reason still not understood, about 6% of people will rupture their other achilles tendon within a year of injury.
Reference
1) Willits K et al. Operative versus nonoperative treatment of acute Achilles tendon ruptures: a multicenter randomized trial using accelerated functional rehabilitation. JBJS 2010; 92: 2767-75. full article. early fxnal rx does better the surgery.
2) Costa ML et al. Randomised controlled trials of immediate weight-bearing mobilisation for rupture of the tendo-Achillis. JBJS Br 2006; 88: 69-77. full article. fxnal rehab nonop vs. casting nonop are equal.
3) Soroceanu A et al. Surgical versus nonsurgical treatment of acute Achilles tendon rupture: a meta-analysis of randomized trials. JBJS 2012; 94: 2136-43. full article. fxnal rehab nonop is as good as surgery with risks.
3) Khan RJ et al. Treatment of acute achilles tendon ruptures. A meta-analysis of randomized, controlled trials. JBJS 2005; 87: 2202-10. full article. classic paper favoring surgery to reduce re-rupture, recognizes higher complication rate.
4) Weber et al. Nonoperative treatment of acute rupture of the achilles tendon: results of a new protocol and comparison with operative treatment. Am J Sports Med 2003; 31: 685-91. full article. another paper supporting surgery to dec rerupture.
5) Wapner KL et al. Repair of chronic Achilles tendon rupture with flexor hallucis longus tendon transfer. Foot Ankle 1993; 14: 443-9. full article. decent outcomes, some lost strength.
6) Bruggeman NB et al. Wound complications after open Achilles tendon repair: an analysis of risk factors. CORR 2004; 427: 63-66. full article. risk for surgical complications.