TFCC TEAR
"Triangular FibroCartilage Complex Tear"
our website is for educational purposes only. the information provided is not a substitution for seeing a medical doctor. for the treatment of a medical condition, see your doctor. we update the site frequently but medicine also changes frequently.
Related articles: broken wrist (distal radius fracture), scaphoid fracture, broken hand, thumb ligament tear
What is a TFCC Tear?
TFCC tear is a injury to a collection of ligaments in your wrist called the "Triangular Fibrocartilage Complex" (aka TFCC).
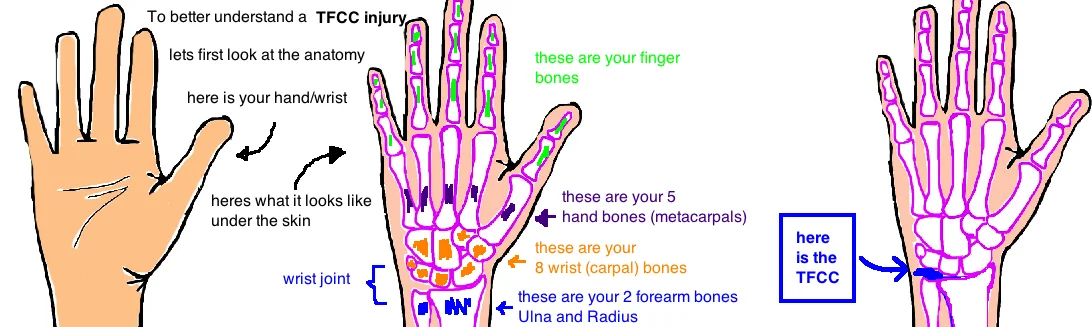
Before we go any further, lets review the anatomy of your TFCC and your wrist.
There are three small ligaments 1) the ulnocarpal ligament, 2) the palmar radiocarpal ligament and 3) the dorsal radiocarpal ligament. There is also a central disk (sort of like the meniscus in the knee).
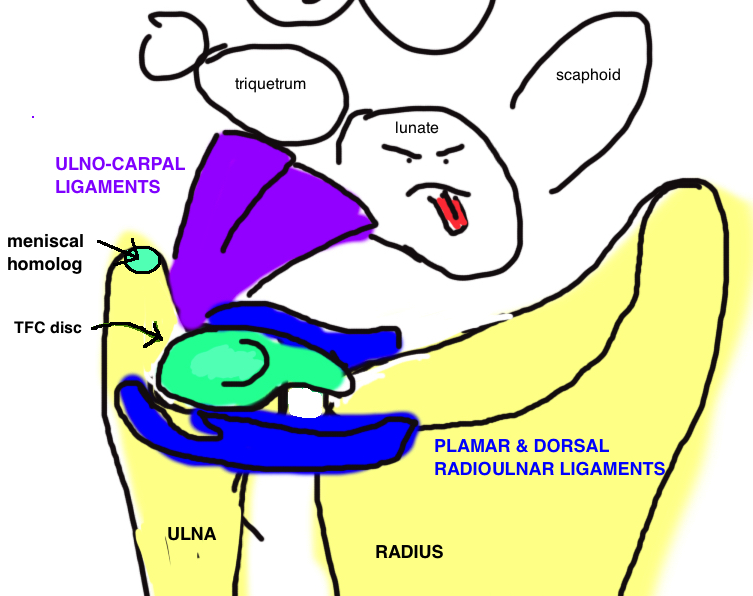
In your forearm there are 2 bones (the radius and ulna) that join up with your 8 wrist bones (aka carpal bones) to form the wrist joint. The two forearm bones also come into contact at your wrist to form the DRUJ (distal radioulnar joint). This joint allows us to rotate our hand from palm up to palm down without moving the rest of our arm. And importantly, this joint is stabilized in part by the TFCC.
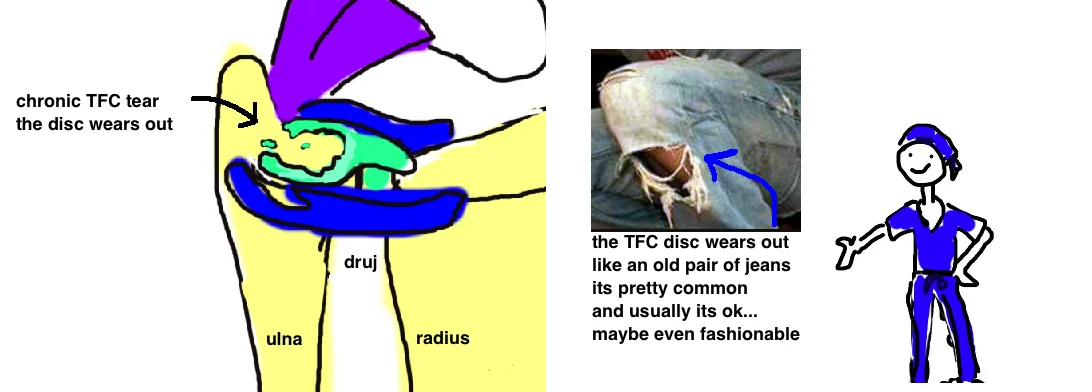
Tears to the TFCC can occur over time from overuse, these are called chronic tears, and this type of tear is very common, with about 50% of people having degenerative cartilage or tears by middle age.
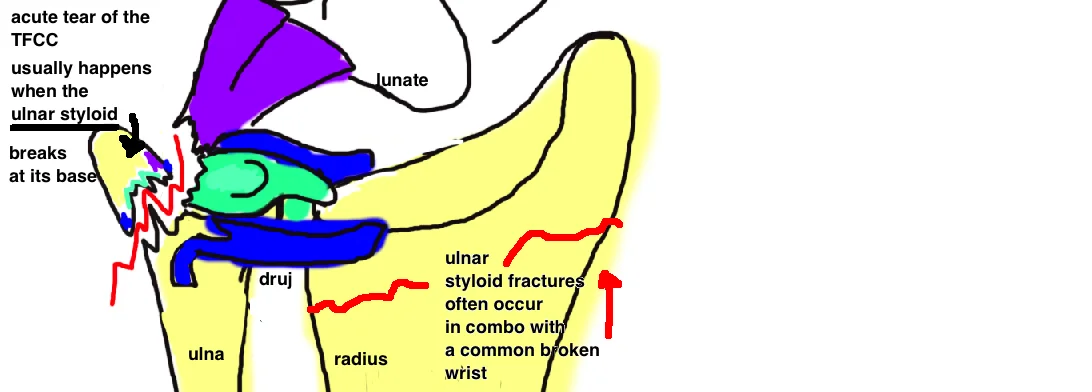
TFCC tears can also be associated with a condition called Ulnar Impaction Syndrome. It usually occurs after an acute trauma to the wrist (you whack your wrist too hard and it tears the TFCC). This occurs in about 20-40% of broken wrists (for more on distal radius fractures, read here), and is particularly concerning when both the distal radius and ulnar styloid is broken. Yet most ulnar styloid fractures don’t cause DRUJ instability because of the dual (front & back) attachments of the TFCC. The ulnar styloid shaft gives attachments for ulnocarpal ligaments and some of the radiocarpal ligaments...but the deep limbs of the radiocarpal ligaments attach to the ulnar head, therefore only when the ulnar styloid is broken at its base are doctors more concerned.

How do you diagnose a TFCC Tear:
A history of symptoms is critical to diagnosis. Common symptoms include ulnar-sided wrist pain (ulnar = small finger side of the wrist), pain worsened by gripping or ulnar deviation. Sometimes you will hear clicking. If there is no joint instability then treatment isn’t required.
X-rays are great at showing broken bones, but they do not demonstrate ligament tears. An MRI can be ordered to show the tear, and oftentimes, a small amount of absorbable dye is injected into the wrist at the time of MRI to give a better picture of the injury.
How do you treat a TFCC Tear?
Most acute TFCC tears don’t require surgical treatment, and even though the ulnar styloid often breaks with a broken wrist, it rarely causes persistent problems like DRUJ instability or chronic pain (this is because only part of the TFCC is attached to the styloid).
Doctors try to manage this injury with rest, immobilization, anti-inflammatory medication (NSAIDs), and sometimes steroid injections.
If pain persists despite the anti-inflammatory treatments, an arthroscopic debridement is recommended. Arthroscopic means using a small camera and mini-tools to clean out the wrist joint an remove any fraying that may be causing inflammation.
In some rare cases of traumatic injury, the TFCC is surgically repaired. Most notably a "Galeazzi Fracture" (see talk) causes wrist instability (specifically the DRUJ), or a large chuck of ulnar styloid gets broken off. This will cause pain and poor function until stability is returned to the wrist.
What is the long term outcome?
This is typically a time limited injury and will resolve with nonsurgical treatment.
The pain usually comes from inflammation, and a recurrence of this inflammation can occur if the wrist is re-injured. Conservative treatment more commonly fails when the wrist is ulna-neutral or even ulna positive (meaning the ulna bone sticks out in the wrist) and this position increases the wear across the wrist.
Overall there are no good studies that show a TFCC tear will lead to future arthritis.
Reference
1. Henry MH. Management of acute triangular fibrocartilage complex injury of the wrist. JAAOS 2008; 16: 320-29. full article. review.
2. Nagle DJ. Evaluation of chronic wrist pain. JAAOS 2000; 8: 45-55. full article. review.
3. Palmer AK. Triangular fibrocartilage complex lesions: a classification. J Hand Surg 1989; 14: 594-606. full article. classic paper defining TFCC and classifying injury.
4. Kirschenbaum D et al. Arthrography of the wrist: assessment of the integrity of the ligaments in young asymptomatic adults. JBJS 1995; 77: 1207-1209. full article. 25% perforations 20-25 yo.
5. Schers TJ, van Heusden HA. Evaluation of chronic wrist pain: arthroscopy superior to arthrography - comparison in 39 patients. Acta Orthop Scand 1995; 66: 540-542. full article.
6. Stuart PR, Berger RA, Linscheid RL, An KN. THe dorsopalmar stability of the distal radioulnar joint. J Hand Surg 2000; 25: 689-699. full article. review anatomic support.
7. Nakamura R et al. The ulnocarpal stress test in the diagnosis of ulnar-sided wrist pain. J Hand Surg Br 1997; 22: 719-23. full article. arthroscopic best dx, physical exam better than mri (79% accurate), xray.
8. Blackwell RE et al. A five-year experience in the treatment of central triangular fibrocartilage complex tears by partial excision. J Hand Surg 2001; 26: 77-84. full article. only 65% good-excellent outcome for persistent pain rx debridement.
9. Haugstvedt JR, Husby T. Results of repair of peripheral tears in the triangular fibrocartilage complex using an arthroscopic suture technique. Scand J Plast Reconstr Surg Hand Surg 1999; 33: 439-447. full article. ok outcomes for tfcc repair.
10. Adams BD, Berger RA. An anatomic reconstruction of the distal radioulnar ligaments for posttraumatic distal radioulnar joint instability. J Hand Surg 2002; 27: 243-251. full article.