BROKEN HAND (METACARPAL FRACTURE)
our website is for educational purposes only. the information provided is not a substitution for seeing a medical doctor. for the treatment of a medical condition, see your doctor. we update the site frequently but medicine also changes frequently.
related topics: broken thumb, broken finger, broken wrist, nailbed injury
What is a Broken Hand (Metacarpal Fracture)?
A broken hand also called a metacarpal bone fracture.
You have five metacarpals bones in your hand, one for each finger (1st is part of your thumb, the 2nd is part of your index finger, the 3rd is part of your middle finger, the 4th part of your ring finger and the 5th part of your pinky finger). When they meet up with your finger bones, they form your knuckles (your knuckles are a joint in your hand that allow for finger motion).
The metacarpal bone is divided into regions: the head, neck, shaft and base. It can break in each of these regions.
A break in the metacarpal neck is the most common, but a metacarpal shaft fracture is also pretty common. A head fracture is less common, and doctors worry about injury to the cartilage within the knuckle when they see this. A base fracture is also less common, and doctors worry about joint dislocation in addition to a break when they see this.
Because the metacarpals form your knuckle, they are commonly broken while punching something. Thats how they got the name the “Boxers Fracture”, which is most commonly a fracture of the 5th metacarpal (your pinky finger). 70% of these occur in people 11 to 45 years old. It’s a young persons injury, typically guys with either too much testosterone or too much alcohol.
How is a Broken Hand (Metacarpal Fracture) diagnosed?
People with a metacarpal fracture will report a specific incident where they injured their hand by punching something hard, or twisting their hand with great force.
Examining the hand will show significant pain and swelling, usually over the knuckle.
Its important to evaluate the position of the fingers as they flex forward to make a fist. In a normal hand, each of the fingers stay in their “lane” and theres no overlap. However, if a metacarpal breaks, it can rotate out of place, which causes the fingers to overlap leading to discomfort and preventing normal grip. This overlap needs to be corrected by straightening out the bone.
Doctors will look at the knuckles for any lacerations. Doctors worry about a "fight bite", meaning the knuckle can get cut against someones tooth during a punch and this causes a high risk for infection (see hand infection talk).
A doctor that is suspicious for a broken hand will then get an x-ray.
X-rays are the best way to diagnose a broken hand. The x-ray will show a crack in the bone, and usually the bone is also bent forward (displaced).
How is a Broken Hand (Metacarpal Fracture) treated?
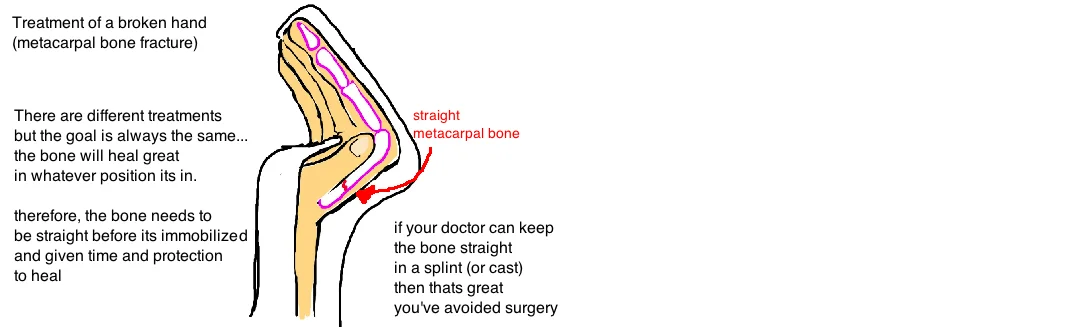
There are different ways to treat a broken hand, and it usually depends on how badly the bone is broken. Some breaks need surgery, while most only need a few weeks in a splint.
When the bone breaks, it usually bends forward too. When it bends too far, the bone is "mal-aligned". This sometimes needs to be straightened out so that the hand heals without future problems. The different fingers can tolerate different degrees of abnormal bending. This stuff can get complicated so we will keep it brief.
Overall if the metacarpal neck breaks, the index and middle finger must be very close to normal, any bending 10-20° beyond normal needs to be straightened (either by pushing & pulling the fracture into place, or with surgery). The ring finger can tolerate a little more bending (about 30-40°) while the pinky finger can tolerate the most (about 50-60°). The pinky tolerates a greater bending deformity because its more flexible so it can compensate for being a little out of position.
If the metacarpal shaft breaks the bone also bends forward. In fact, our hand is less tolerant of a bent shaft and therefore it usually needs to be straightened. A broken shaft can also rotate as described above, and this needs to be corrected also.
So which breaks need surgery? It all depends on how stable the broken hand is.
Nonsurgical treatment is always preferred. If the broken bone is stable, and it will stay in place with a splint, then a splint is worn for 2-3 weeks, and then removed so people can slowly start using the hand again. For bad breaks, an extra 2 weeks in a cast is needed. But full activity (including sports) is typically allowed after 4-6 weeks.
The hand is usually splinted in a specific position: the wrist extended 30° and the fingers flexed about 90°, to prevents stiffness of the collateral ligaments (ligaments holding the finger and metacarpal bones together), as well as takes tension of the lumbrical muscles, which can act as a deforming force on the fracture (meaning, the pull of this muscle makes the fracture more deformed).
If the bone is too unstable (meaning the bone wont stay straight) to heal in a splint, then doctors typically recommend surgery. The surgeon will realign the broken bone and then use two pins (which are removed in about 3 weeks) or small screws (which will stay in forever) to hold the bones in this good alignment. The metal is used to give stability to the unstable broken bone.
What is the long term outcome?
Why is it so important to straighten out the bone?
If a metacarpal heals excessively bent, it will develop clawing of the fingers (actually its called "pseudoclawing") by changing the biomechanics of the finger tendons (the fingers will extend at the MCP joints to compensate for the MC head which is flexed into the palm, this will increase the tension of the finger flexors and give the finger a sort of claw like appearance.)
Additionally, the bent bone will be felt as a hard bump in the palm of your hand. This can prevent full grip strength.
Lastly, if the finger is rotated, then when you make a fist, the finger will tuck under the others causing an uncomfortable grip.
Once the cast comes off or the pins come out (depending on the treatment), you need to start moving the finger to prevent stiffness.
Oftentimes people will meet with a hand therapist to review exercises to do every day to prevent this stiffness. Full recovery depends on the patient and the severity of injury. Usually the pain will subside within the first two weeks. The pain from the bones rubbing together will stop because the body has formed a callus, or a shell around the fracture to hold everything in place and to bridge the gap with new bone.
Hand function starts to approach near normal in about 2 months, however, it can take up to 6 months to truly feel like your hand is back to its old self after this injury.
Reference
1. Elfar J, Mann T. Fracture-dislocations of the proximal interphalangeal joint. JAAOS 2013; 21: 88-98. full article. review
2. Chung KC, Spilson SV: The frequency and epidemiology of hand and forearm fractures in the United States. J Hand Surg Am 2001; 26:908-915. see article. general facts. pinky finger is 40% of hand injuries, then other 4 get equal distribution. prox phalanx most injured, then distal then middle.
3. Dabezies EJ, Schutte JP: Fixation of metacarpal and phalangeal fractures with miniature plates and screws. J Hand Surg 1986;11:283–288. see article. 90% normal ROM in 25 MC and 27 phalanx fx after ORIF. good outcome data.
4. Page SM, Stern PJ. Complications and range of motion following plate fixation of metacarpal and phalangeal fractures. J Hand Surg 1998;23: 827–832. see article. 100 MC, 100 phalanx fx after ORIF, only 76% got >200 deg motion for MC (but only 11% in phalanx fx). plate req. inc soft tissue dissection, tissue adheres to plate.
5. Diwaker HN, Stothard J. The role of internal fixation in closed fractures of the proximal phalanges and metacarpals in adults. J Hand Surg Br 1986; 11:103–108. see article. compared 50 k-wire and orif vs 50 nonop rx. orif best motion (80% got 200 deg motion) vs only 50% in k-wire, nonop.
6. Botte MJ et al. Complication of smooth pin fixation of fracture and dislocation in the hand and wrist. CORR 1992: 276:194-201. see article. complications w. K-wire: 18% overall: 7% infxn; 5% nonunion, 4% pin loosening. main concern k-wire is osteomyelitis and lost reduction, extensor mech tethering.
7. Galanakis I et al. Treatment of closed unstable metacarpal fractures using percutaneous transverse fixation with Kirschner wires. J Trauma 2003; 55:509-513. see article. pin to neighboring MC, one prox, two distal. keep for 4 wks (3 isnt enough). good outcomes.
8. Henry MH. Fractures of the Proximal Phalanx and Metacarpals in the Hand: Preferred Methods of Stabilization. JAAOS 2008; 16: 586-595. see article. eview.